
Thyroid Cancer
Most Thyroid Swellings Are Not Cancer—
But Every Lump Deserves Expert Evaluation.
A thyroid swelling is one of the commonest reasons people visit an endocrine or head & neck surgeon. While most thyroid lumps are completely harmless, a small proportion require treatment. The goal of evaluation is not simply to diagnose cancer—but to identify who truly needs surgery, who can be safely observed, and who will benefit from long-term follow-up. The encouraging news is that even when a thyroid nodule turns out to be cancerous, the vast majority are highly curable with appropriate treatment and follow-up.
Understanding Thyroid Nodules and Thyroid Cancer
Thyroid nodules are among the most common endocrine disorders, affecting 20–76% of adults, especially with increasing age and the widespread use of ultrasound. Fortunately, 80–85% of thyroid nodules are completely benign, and only 5–15% are found to be thyroid cancer after appropriate evaluation.
Thyroid nodules are up to four times more common in women than men. However, when a thyroid nodule occurs in men, the likelihood of malignancy is relatively higher. This is why every thyroid swelling deserves expert evaluation, regardless of its size or symptoms.
Perhaps the most reassuring fact about thyroid cancer is that, when diagnosed early, it is one of the most curable cancers. Most thyroid cancers are slow growing, highly curable, and have a 5-year survival rate approaching 98–100%, depending on the tumour type, stage, age and extent of disease. With timely surgery and appropriate follow-up, the overwhelming majority of patients go on to live completely normal lives.
Not all thyroid cancers behave in the same way. Fortunately, papillary and follicular thyroid cancers account for the vast majority of cases and are associated with excellent long-term outcomes. Medullary thyroid cancer is less common and requires a different treatment approach, while anaplastic thyroid cancer is rare but more aggressive. Knowing the exact type of thyroid cancer helps us recommend the most appropriate treatment and predict long-term outcomes.
When Does a Thyroid Lump Need Expert Evaluation?
Although most thyroid nodules are harmless, certain features increase the likelihood of thyroid cancer and warrant prompt evaluation. Early evaluation does not always mean early surgery—it means making the right diagnosis before deciding whether any treatment is necessary.
- A history of radiation exposure to the head or neck during childhood
- Rapidly enlarging thyroid swelling
- A family history of thyroid cancer or inherited endocrine syndromes
- Suspicious findings on neck ultrasound
- Enlarged cervical lymph nodes associated with a thyroid nodule
- Hoarseness of voice or difficulty swallowing accompanying a thyroid swelling
It is important to remember that these warning signs do not automatically indicate thyroid cancer. They simply identify patients who should undergo a more detailed evaluation. Early assessment allows accurate diagnosis, timely treatment when required, and equally importantly, reassurance for the many patients whose thyroid nodules prove to be benign.
How Is Thyroid Cancer Diagnosed?
No single test can diagnose every thyroid nodule. Each investigation answers a different question—whether the swelling is benign or cancerous, how far it has spread, and what treatment, if any, is actually required. In many patients, a thyroid nodule is discovered incidentally during a routine health check-up or while undergoing an ultrasound or CT scan for another reason. However, not every thyroid nodule requires FNAC or surgery. The decision depends on the ultrasound appearance, size and individual risk factors.
The goal of evaluation is not simply to determine whether a nodule is cancerous, but also to identify whether the nodule needs any immediate surgical attention or can be safely watched. Most patients require only ultrasound and FNAC to establish the diagnosis. Additional investigations are reserved for selected patients where they are likely to influence treatment planning.
Diagnosis usually follows a stepwise approach:
Clinical Examination
⬇
High-resolution Neck Ultrasound
⬇
Ultrasound-guided FNAC
⬇
CT / MRI / PET-CT (selected patients only)
Every patient should be assessed individually so that treatment is based on both tumour biology and patient factors, rather than the thyroid nodule alone.
Risk Stratification — Not Every Thyroid Cancer Is the Same
Not all thyroid cancers behave in the same way. Some require only limited surgery, while others need a more comprehensive approach. Choosing the right treatment begins with understanding both the patient and the tumour. Factors that influence treatment include:
| Patient Profile | Cancer Characteristics |
| Age | Size |
| Sex | Subtype |
| Previous Surgery | Extent |
| Family history | Nodal or Distant Metastasis |
Thyroid cancer is one of the very few cancers in which age directly influences staging and prognosis. Younger patients usually have an excellent outlook, while cancers occurring at the extremes of age may require closer monitoring and more intensive treatment.
The goal is simple—achieve the highest cure rates while preserving quality of life and avoiding unnecessary treatment whenever it is safely possible. Every decision is individualized because no two thyroid cancers are exactly alike.
Treatment Journey of Thyroid Cancer
Successful treatment extends beyond the operation itself. Every patient follows a carefully planned pathway that includes surgery, individualized postoperative treatment and long-term surveillance.
1. Surgery
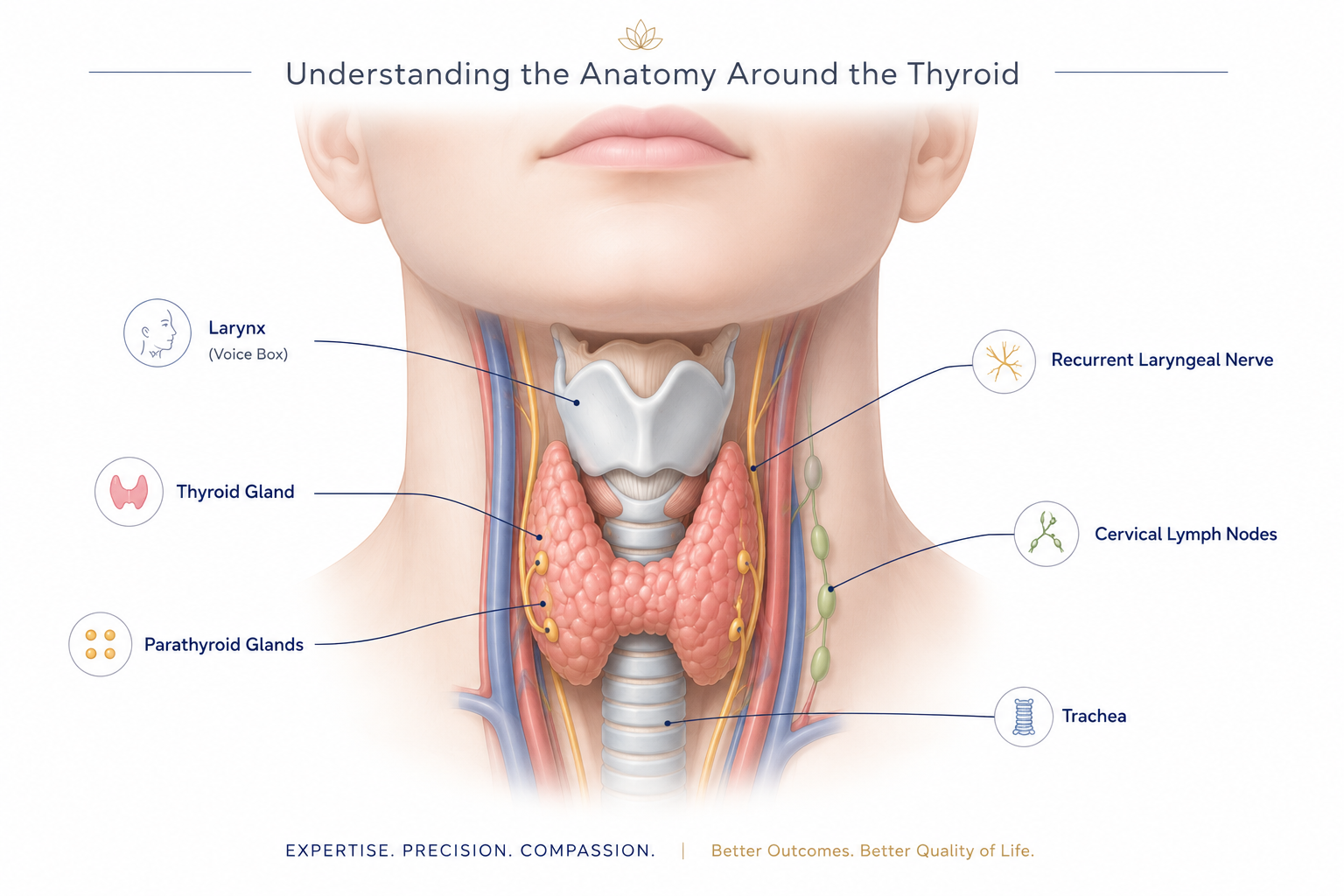
Surgery is the cornerstone of treatment for most thyroid cancers. However, successful thyroid cancer surgery is not measured simply by removing the cancer. It is equally defined by preserving the voice, protecting the parathyroid glands, maintaining normal calcium balance and ensuring the best possible quality of life. When thyroid cancer has spread to the lymph nodes, neck dissection may also be required to achieve complete disease clearance. Every operation is individualized to provide the best oncological outcome while preserving important structures such as the recurrent laryngeal nerves and parathyroid glands whenever safely possible.
2. Risk Assessment & Radioactive Iodine Therapy
Following surgery, the biopsy report is carefully reviewed to determine the risk of recurrence into low, intermediate and high. Not every patient requires radio iodine treatment.
Patients with low-risk differentiated thyroid cancers often require no further therapy beyond surgery. However, patients with intermediate or high-risk disease, residual thyroid tissue or metastatic disease may be evaluated first by Radio Iodine scan and tumor markers for the need of Radio Iodine Therapy (RAI).
Radioactive Iodine (RAI) therapy, which destroys microscopic thyroid tissue and remaining iodine-avid cancer cells, further reducing the risk of recurrence. Radioactive iodine is unique to differentiated thyroid cancers such as papillary and follicular thyroid cancer and is not required for every patient.
3.Recovery & Thyroid Hormone Management
Recovery following thyroid surgery is generally smooth, and most patients return to their normal routine within a few weeks. Patients undergoing total thyroidectomy require lifelong thyroid hormone replacement, while many patients who undergo hemithyroidectomy continue to produce sufficient thyroid hormone naturally.
In addition to replacing the body’s normal hormone requirements, thyroid hormone tablets may also be used to maintain the Thyroid Stimulating Hormone (TSH) at an appropriate level in selected patients. This strategy, known as TSH suppression, helps reduce the risk of recurrence in patients with intermediate or high-risk thyroid cancer and is individualized according to the patient’s risk profile and response to treatment.
4. Long-Term Surveillance
One of the greatest advantages of differentiated thyroid cancer is that treatment response can be monitored with remarkable accuracy.
Regular follow-up usually includes:
- Clinical examination
- Neck ultrasonography
- Serum thyroglobulin (Tg)
- Anti-thyroglobulin antibodies (Anti-Tg Ab)
These investigations form the basis of Dynamic Risk Stratification (DRS), allowing treatment recommendations to evolve according to the patient’s response over time.
When required, additional investigations such as a diagnostic radioactive iodine whole-body scan, CT or PET-CT may be performed to evaluate suspected recurrent disease and guide further treatment.
This ability to accurately monitor treatment response over time is one of the unique reasons why differentiated thyroid cancers have such excellent long-term outcomes
Life After Thyroid Cancer Treatment
Most patients return to a completely normal, healthy and active life after successful treatment for thyroid cancer. Long-term care focuses on maintaining normal hormone levels, detecting recurrence early and helping patients enjoy an excellent quality of life.
Depending on the type of surgery performed, some patients may require lifelong thyroid hormone replacement, while others continue to produce sufficient thyroid hormone naturally.
Regular follow-up allows treatment to be individualized according to each patient’s ongoing response rather than using a one-size-fits-all approach.
Patients are encouraged to:
✓ Take thyroid medication regularly
✓ Attend scheduled follow-up visits
✓ Maintain adequate calcium and vitamin D intake when advised
✓ Follow a healthy balanced diet
✓ Remain physically active
✓ Report any new neck swelling or voice change promptly
FAQ’s
Can thyroid cancer be cured?
Yes. Most differentiated thyroid cancers have an excellent prognosis, with cure rates exceeding 95% when treated appropriately.
Will I need lifelong medicines?
Patients undergoing total thyroidectomy usually require lifelong thyroid hormone replacement. Those undergoing hemithyroidectomy may not require medication if the remaining thyroid functions normally.
Can thyroid cancer come back?
Although recurrence can occur in a small proportion of patients, regular follow-up enables early detection and effective treatment in most cases.
Will my voice change permanently?
Temporary voice changes may occur after surgery, but permanent voice problems are uncommon when surgery is performed carefully while preserving the recurrent laryngeal nerves. With recent advances in technology, the surgery is being performed using a IONM (intra operative nerve monitoring) which continuously guides on to the status of the nerve resulting in safe surgery.
Can women become pregnant after thyroid cancer treatment?
Yes. Most women can safely conceive after completing treatment and achieving stable thyroid hormone levels under medical supervision. However post RAI therapy, ideally one should be waiting for at least 6 months before planning pregnancy.
Is radioactive iodine required for everyone?
No. Radioactive iodine is recommended only for selected patients based on the tumour stage and recurrence risk
Worried About a Thyroid Swelling?
Most thyroid nodules are harmless, but the key is obtaining the correct diagnosis early. Expert evaluation helps distinguish patients who simply need reassurance from those who benefit from timely treatment.
Whether you have a newly diagnosed thyroid nodule, an indeterminate biopsy, confirmed thyroid cancer or recurrent disease, a personalized treatment plan offers the best opportunity for cure while preserving long-term quality of life.
Schedule a consultation for:
✓ Thyroid nodules
✓ Thyroid cancer
✓ Second opinions
✓ Recurrent thyroid cancer
✓ Scarless thyroid surgery (selected patients)