
Pharyngeal Cancer Treatment
Choosing the Right Treatment, Not Just the Right Operation
Unlike many other head and neck cancers, treatment of pharyngeal cancers often begins with the goal of preserving the voice, swallowing and normal throat function. Surgery is not always the first treatment. Careful evaluation helps determine whether radiation therapy, chemoradiation or surgery offers the best chance of cure with the best quality of life.
Understanding Pharyngeal Cancer
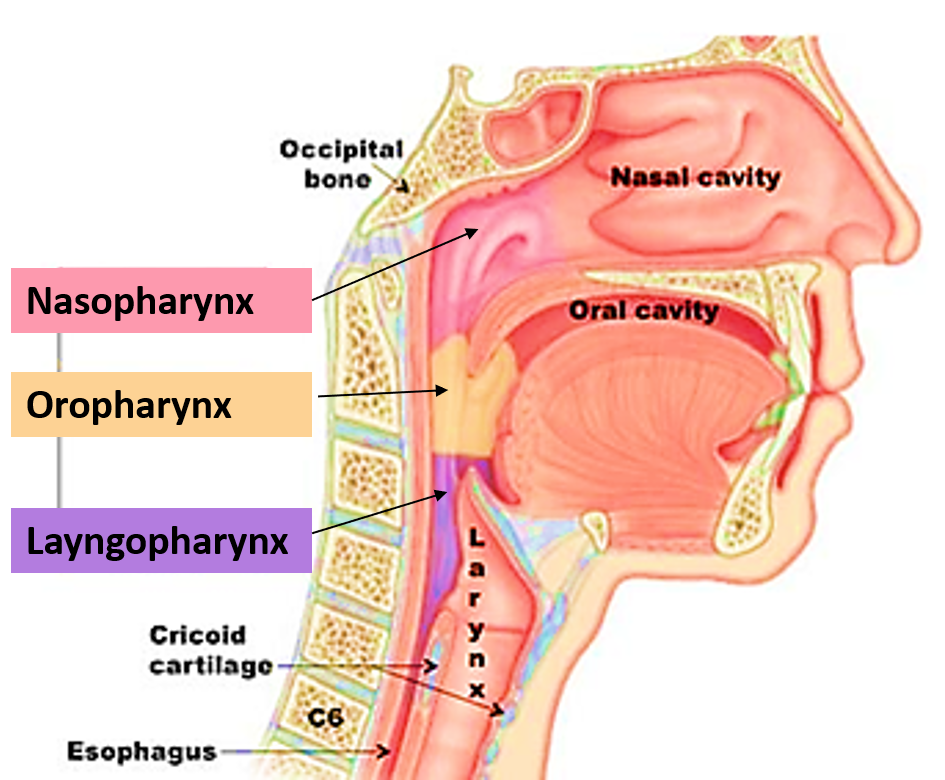
The pharynx, commonly called the throat, is divided into three different regions:
• Nasopharynx (behind the nose)
• Oropharynx (tonsils, base of tongue and soft palate)
• Hypopharynx (lower throat behind the voice box)
Although these cancers occur within the same organ, they differ significantly in their causes, behaviour and treatment. Accurate diagnosis is therefore essential before deciding the most appropriate treatment.
Symptoms of Pharyngeal Cancer
Symptoms often depend on the part of the throat involved and may include:
- Persistent sore throat
- Difficulty or pain while swallowing
- Lump in the neck
- Ear pain without ear disease
- Change in voice
- Nasal blockage or nosebleeds
- Blood in saliva
- Unexplained weight loss
- Persistent bad breath
Many patients initially mistake these symptoms for recurrent throat infections. Symptoms persisting beyond two to three weeks should always be evaluated by a Head and Neck Cancer Specialist.
How Is Pharyngeal Cancer Diagnosed?
Successful treatment begins with accurate diagnosis and precise staging.
Clinical Consultation
A detailed history and examination help understand the duration of symptoms, swallowing function, voice changes, tobacco exposure, sexual practices and previous medical illnesses.
Flexible Video Endoscopy
One of the most important investigations for pharyngeal cancers is flexible nasopharyngolaryngoscopy. A thin flexible camera is passed comfortably through the nose to examine the entire throat under magnified vision. This allows accurate assessment of tumour location, size, vocal cord movement and airway without causing significant discomfort. The procedure usually takes only a few minutes and is performed in the outpatient clinic. This evaluation also allows taking a biopsy for the confirmation.
Imaging
Depending on the tumour, investigations may include:
- Contrast CT Scan
- MRI
- PET-CT Scan
These studies determine the exact extent of disease, lymph node involvement and possible distant spread before treatment planning.
Biopsy
A tissue diagnosis is mandatory before treatment begins. Depending on tumour location, biopsy may be performed under local or general anaesthesia.
Choosing the Right Treatment
Unlike oral cancer, surgery is not automatically the first treatment for most pharyngeal cancers.
Treatment decisions are individualized after considering:
- Exact tumour location
- Stage of disease
- HPV or EBV status where applicable
- Voice and swallowing function
- Patient age and fitness
- Expected quality of life after treatment
Whenever appropriate, cases are discussed in a multidisciplinary tumour board involving Head & Neck Surgeons, Radiation Oncologists, Medical Oncologists, Radiologists and Pathologists to develop the most effective treatment strategy.
Organ Preservation – The Modern Treatment Philosophy

One of the greatest advances in head and neck oncology has been the ability to cure many pharyngeal cancers without removing major organs. For appropriately selected patients, radiation therapy alone or combined chemoradiation can provide cure rates comparable to surgery while preserving natural speech, swallowing and appearance. This approach is known as organ preservation and has become the standard of care for many pharyngeal cancers worldwide.
Throughout treatment, patients are closely monitored to ensure the cancer responds adequately. If complete response is achieved, surgery can often be avoided altogether.
Organ preservation is an excellent treatment strategy for appropriately selected patients. However, when the tumour is very advanced or does not respond adequately to treatment, surgery may provide the best chance of cure. Every treatment recommendation is individualised after careful multidisciplinary discussion or Tumor Board Discussion.
When Is Surgery Required?
Although many pharyngeal cancers are treated without surgery initially, surgery continues to play a vital role in selected situations.
Surgery may be recommended:
- Early cancers suitable for TORS minimally invasive/robotic removal
- Residual disease after radiation or chemoradiation
- Cancer recurrence after previous treatment
- Persistent metastatic lymph nodes in the neck
- Selected advanced tumours where surgery offers the best chance of cure
Modern surgical techniques aim to achieve complete cancer clearance while preserving swallowing, speech and appearance whenever safely possible.
Treatment Based on Tumour Location
Nasopharyngeal Cancer
Nasopharyngeal cancer develops behind the nose and differs significantly from other head and neck cancers. It is strongly associated with Epstein-Barr Virus (EBV) and is highly sensitive to radiation therapy.
Because of its deep location close to the skull base and major nerves, surgery is rarely the primary treatment. Most patients are successfully treated with radiation therapy alone or combined chemoradiation depending on disease stage.
Surgery is generally reserved for persistent or recurrent disease after completion of radiation therapy, where carefully selected salvage procedures may offer long-term disease control.
Oropharyngeal Cancer
The oropharynx includes the tonsils, base of tongue and soft palate. Increasingly, these cancers are related to Human Papilloma Virus (HPV), particularly among younger individuals without significant tobacco exposure.
Treatment depends on tumour size, HPV status and lymph node involvement. Many patients achieve excellent cure rates with organ-preserving chemoradiation.
Selected early tumours may also be treated using minimally invasive transoral surgery, allowing complete tumour removal without external incisions. Surgery may also be recommended as salvage treatment for persistent or recurrent disease following radiation.
Hypopharyngeal Cancer
Hypopharyngeal cancers arise in the lower throat and often present at a more advanced stage because early symptoms may be subtle.
Treatment usually involves combined chemoradiation with the aim of preserving swallowing and voice whenever feasible.
In advanced disease causing airway obstruction or poor response after chemoradiation, salvage surgery may become necessary. Depending on tumour extent, surgery may involve removal of part or all of the voice box and pharynx followed by complex reconstruction to restore swallowing.
Nutrition During Treatment
Maintaining nutrition is one of the most important factors influencing successful treatment. Patients receiving radiation therapy or chemoradiation often experience painful swallowing, reduced taste sensation, dry mouth and weight loss. Good nutritional support helps maintain body weight, reduces treatment interruptions, improves healing and decreases complications.
Where oral intake becomes inadequate, temporary feeding tube support may be recommended to ensure uninterrupted nutrition throughout treatment. Nutrition is not an optional part of treatment—it is an essential component of cancer care.
Recovery and Long-Term Follow-Up
Treatment does not end when radiation or surgery is completed. Regular follow-up helps monitor recovery, detect recurrence early and manage long-term effects such as swallowing difficulty, dry mouth, neck stiffness or thyroid dysfunction.
Speech therapy, swallowing rehabilitation, nutritional counselling and physiotherapy are often important components of recovery. Most patients gradually return to normal daily activities over the months following treatment.
Frequently Asked Questions
Is surgery always required for pharyngeal cancer?
No. Many pharyngeal cancers are treated successfully with radiation therapy or combined chemoradiation without surgery.
Why isn’t surgery the first treatment?
Removing parts of the throat can permanently affect speech and swallowing. When radiation or chemoradiation can provide similar cure rates while preserving these functions, non-surgical treatment is generally preferred.
Will I lose my voice?
Most patients treated with organ-preserving therapy retain their natural voice. Voice changes during treatment are common but often improve over time.
Will I be able to swallow normally again?
Most patients recover swallowing function after treatment, although rehabilitation and swallowing exercises may be required during recovery.
Will I need a feeding tube?
Not everyone. Feeding tubes are used when swallowing becomes inadequate during treatment to maintain nutrition and allow uninterrupted therapy. They are usually temporary.
Can pharyngeal cancer come back?
Yes. Even after successful treatment, recurrence remains possible. Regular follow-up examinations allow early detection and improve the chances of successful salvage treatment.
What happens if the cancer comes back?
Treatment depends on where the recurrence occurs and previous treatments received. Surgery often becomes the preferred option for recurrent disease after radiation therapy.
Is HPV-related throat cancer different?
Yes. HPV-positive oropharyngeal cancers generally respond better to treatment and usually have an excellent prognosis compared with HPV-negative cancers.
Can I eat normally after treatment?
Most patients gradually return to a normal diet, although recovery may take several weeks or months depending on treatment intensity. Swallowing therapy and nutritional guidance can significantly improve recovery.
Can pharyngeal cancer be cured?
Yes. Many pharyngeal cancers are curable, particularly when diagnosed early and treated appropriately. Even advanced cancers can often be successfully managed using modern multidisciplinary treatment approaches.
The Right Treatment Matters
Not every pharyngeal cancer requires surgery, and not every patient benefits from the same treatment. Careful evaluation allows the treatment to be tailored to the disease, balancing the highest chance of cure with preservation of speech, swallowing and quality of life.
Because the best treatment is the one that is right for you.